





Abstract
The new guidelines of the HerniaSurge group recommend that only an expert hernia surgeon should repair a re-recurrent inguinal hernia. We report the efficacy of the hybrid method with explorative laparoscopy and anterior open approach for re-recurrent inguinal hernia repair. A 61-year-old man underwent anterior open preperitoneal mesh repair for right inguinal direct hernia and laparoscopic transabdominal preperitoneal repair for recurrence. Two years after the second surgery, re-recurrent inguinal hernia was confirmed. We carried out explorative laparoscopy for the re-recurrent inguinal hernia, which revealed a re-recurrent hernia orifice. We performed the anterior open approach while observing from the abdominal cavity. Explorative laparoscopy can help in accurately determining the orifice of the re-recurrent inguinal hernia. Based on that information, the hernia sac can be reached through the shortest route using the anterior open approach.
INTRODUCTION
According to the new guidelines of the HerniaSurge group, the recurrence rate of inguinal hernia reaches 15% [1]. Laparoscopic repair for recurrence after primary anterior open repair and anterior open repair for recurrence after laparoscopic primary repair are recommended for recurrent inguinal hernia. The re-recurrence frequency of inguinal hernia repair, in accordance with the guidelines, was reported as 1.0–1.2% on 1-year follow-up [2]. However, these guidelines recommend that only an expert hernia surgeon should repair a re-recurrent inguinal hernia after a failed anterior and posterior repair, and the choice of technique depends on patient- and surgeon-specific factors.
We report the efficacy of the hybrid method with explorative laparoscopy and anterior open approach for managing re-recurrence after previous anterior and posterior inguinal hernia repair.
CASE REPORT
A 61-year-old man underwent anterior open preperitoneal mesh repair (direct Kugel method) for right inguinal direct hernia. Recurrence was confirmed 5 years after surgery and was managed through laparoscopic transabdominal preperitoneal repair (TAPP). The recurrent hernia orifice was confirmed on the medial side of the previous mesh placed in the preperitoneal cavity. The mesh plug was placed and fixed in this orifice by the preperitoneal approach. The patient experienced symptomatic re-recurrence 2 years after the second surgery. To confirm the re-recurrent hernia orifice, we first carried out explorative laparoscopy, which revealed a re-recurrent hernia orifice between the mesh at the primary repair and the mesh plug at the secondary repair by TAPP (Fig. 1). Because dissecting between them seemed difficult, the anterior open approach was performed. The skin was incised just above the hernia orifice. The hernia sac was easily confirmed because it protruded with abdominal air pressure (Fig. 2). After the tissues along the hernia sac were dissected, the transverse fascia covering the sac was incised, the preperitoneal cavity was confirmed, and the mesh plug was removed. Sufficient space was secured in the preperitoneal cavity from the medial edge of the previous mesh to the dorsal side of the pubis. The Prolene Hernia System (PHS®; Ethicon, Norderstedt, Germany) with bilayer was used for repair. While observing from the abdominal cavity, we confirmed that the position of the inlay mesh of the PHS in the preperitoneal cavity was appropriate (Fig. 3). Subsequently, the onlay mesh of the PHS was fixed on the transverse fascia (Fig. 4). The postoperative course was free of complications.
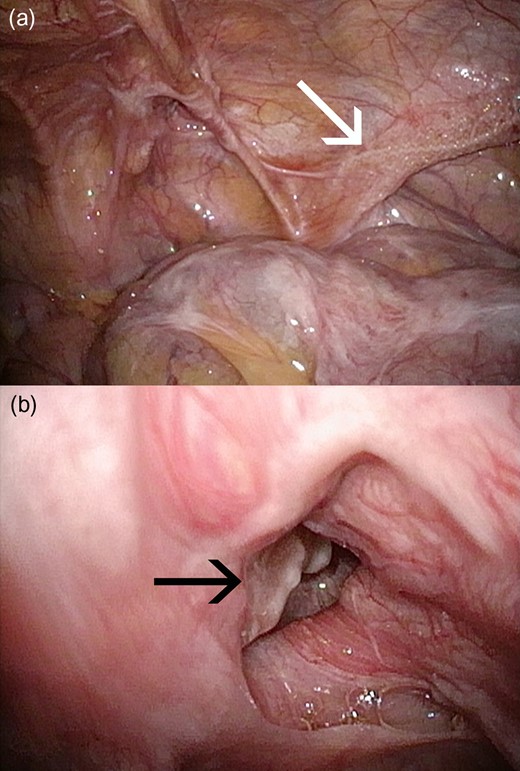
(a) The re-recurrent hernia orifice was confirmed between the mesh (white arrow) at the primary repair and the mesh plug at the secondary repair by transabdominal preperitoneal repair. (b) The mesh plug (black arrow) at the secondary repair got detached from the outside and migrated into the preperitoneal cavity.
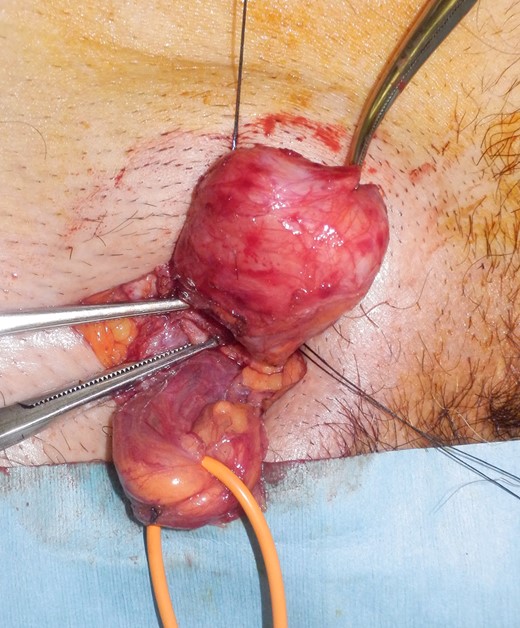
The hernia sac was easily confirmed because it protruded with abdominal air pressure.
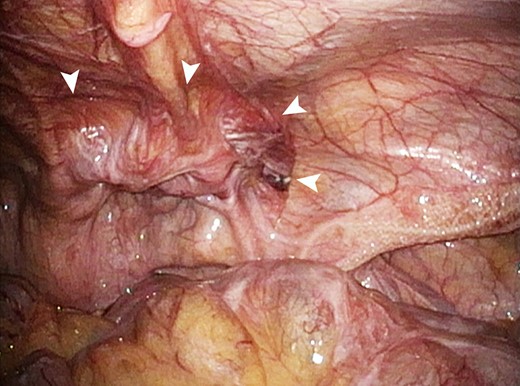
By observing from the abdominal cavity, the position of the inlay mesh (arrow head) in the preperitoneal cavity was confirmed to be appropriate.
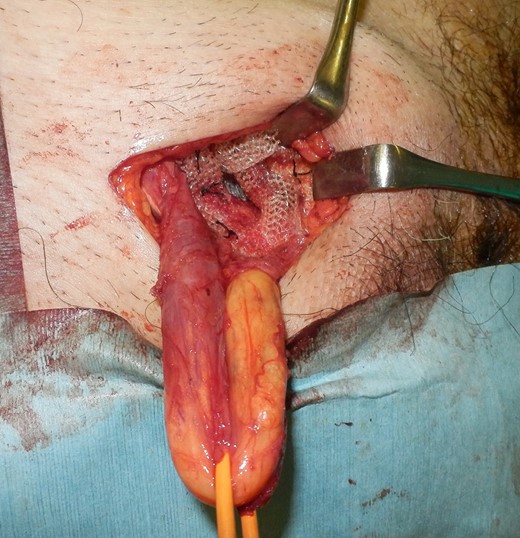
The onlay mesh was fixed on the transverse fascia.
DISCUSSION
Explorative laparoscopy can accurately reveal the orifice of re-recurrent inguinal hernia. Based on that information, the hernia sac can be reached using the shortest route through the anterior open approach.
Explorative laparoscopy can determine the position and size of the orifice of re-recurrent inguinal hernia from the abdominal cavity. Because the hernia sac protrudes because of abdominal air pressure, the hernia orifice is easily visible from the abdominal cavity. Even if tissues adhered to the hernia orifice, the position of the hernia orifice can be identified by compressing the top of the hernia from the outside of the body toward the abdominal cavity.
For recurrent or re-recurrent inguinal hernia, minimum skin incision is preferred. It is important to reach the top of the hernia sac with the shortest route and to expose the hernia sac with minimal dissection. The protrusion of the hernia sac due to abdominal air pressure makes it easy to dissect from the surrounding tissue. In the inguinal canal, the structure is difficult to identify because of severe adhesions from previous surgery. Furthermore, it is important to identify the hernia sac rather than the spermatic cord. Since a relatively loose connective tissue is present around the hernia sac, the hernia orifice could be easily reached by dissecting around the sac.
After identifying the hernia orifice and incising the transverse fascia covering the sac, the situation of the preperitoneal cavity is confirmed. In this case, the space of the preperitoneal cavity was sufficiently secured and the inlay mesh of the PHS could be placed. The position of the inlay mesh from the abdominal cavity can be confirmed by the laparoscope.
The re-recurrence rate of inguinal hernia repair in accordance with the guidelines is reported as 1.0–1.2% on 1-year follow-up [2]. However, according to a nationwide 8-year follow-up study, there were 2117 reoperations (3.1%) and 187 re-reoperations (8.8%) after 67 306 primary hernia repairs [3]. It seems that the re-recurrence rate of inguinal hernia repair is further increasing in the subsequent years. There is very little information in the literature about re-recurrent inguinal hernia repair. Kockerling et al. [4] reported that explorative laparoscopy is an important decision tool for re-recurrent inguinal hernia treatment to minimize the risks of the procedure for the patients. They performed explorative laparoscopy for three cases of re-recurrence after anterior and posterior inguinal hernia repair. In one case, TAPP was relatively easy to perform, and in the remaining two cases, anterior open repair was selected for severe adhesions.
Dissecting preperitoneal cavity adhesion through the laparoscopic technique only or confirming the hernia sac and orifice with minimal adhesion dissection through the anterior open approach only may be difficult. After identifying the situation of the hernia orifice from the abdominal cavity by explorative laparoscopy, performing the anterior open approach with minimal skin incision and minimal adhesion dissection is useful. The hybrid method with explorative laparoscopy and the anterior open approach is useful for re-recurrent inguinal hernia.
CONSENT FOR PUBLICATION
Written consent was obtained from the patient for publication of this article.
ACKNOWLEDGEMENTS
We would like to thank Editage (www.editage.jp) for English language editing.
CONFLICT OF INTEREST STATEMENT
The authors have no disclosure or conflict of interest related to this article.
FUNDING
There were no sponsors participating in this case report.

{kind=link}
{kind=link}
{kind=link}
{kind=link}