





Abstract
Capsule endoscopy (CE) is commonly used for examining and diagnosing gastrointestinal disease, especially small bowel disease. Capsule retention is a well-known and significant complication of CE and requires surgical or endoscopic removal. Most reports described the retrieval of retained CE via laparotomy. We report a case of successful retrieval of the capsule using laparoscopic surgery.
INTRODUCTION
Capsule endoscopy (CE) is increasingly used for the evaluation of small bowel disease. The ease of use and patient tolerance of CE has made it popular among gastroenterologists and patients. Currently, CE is most commonly used to identify the origin of obscure gastrointestinal bleeding, but its indications are broadening [1]. Various reports have described impaction or retention of the capsule in the small bowel that required retrieval [2]. Despite the low risk of complications [3], capsule retention occurs in 1–3% of cases. Capsule retention may reveal the underlying cause of the gastrointestinal disease, but can cause acute intestinal obstruction and perforation requiring surgery [4]. Here, we describe a case of retained capsule that was retrieved with laparoscopic surgery.
CASE REPORT
A 66-year-old male had a history of pain in peri-umbilical region and with a history of long term use of analgesics drugs. Laboratory data showed a hemoglobin level of 9 g/dl and a positive fecal occult blood.
The cause of the gastrointestinal bleeding could not be determined despite CECT abdomen UGI endoscopy and colonoscopy. The small bowel was therefore imaged using CE. The images of CE showed multiple circumferential strictures with ulcerated Mucosa in ileal region.
The patient was unable to pass the capsule more than 4 weeks after ingestion and developed sub acute intestinal obstruction.
Abdominal X-ray showed the retained capsule in the right side of the abdomen (Fig. 1). Colonoscopy was normal.
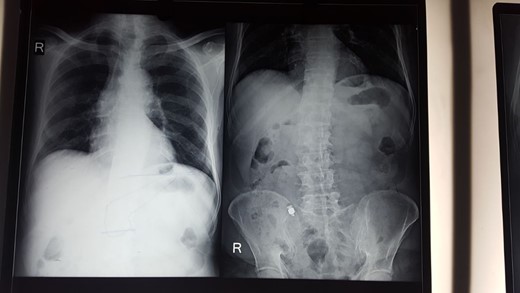
X-ray abdomen shows capsule in right lower abdomen.
Patient planned for diagnostic laparoscopy.
After diagnostic laparoscopy small bowel revealed a stricture in the terminal ileum 3 feet proximal to the ileocecal valve. With the help of C-arm machine video capsule identified (Fig. 2).
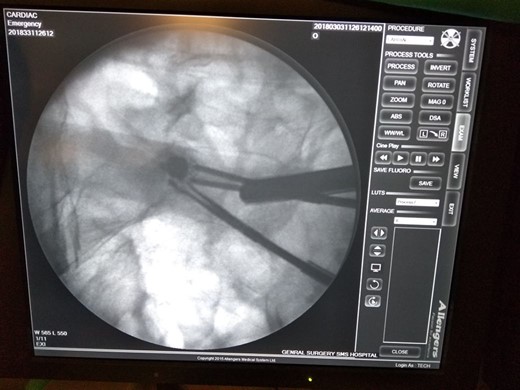
C-arm image.
Retained video capsule removed (Fig. 3) and stricturoplasty done extracorporeally by taking out the loop through an incision in right iliac region. Patient discharged on Day 7 with liquid diets. Post-operative picture of patient (Fig. 4).

Removal of retained video capsule endoscope.
Post-operative picture.
DISCUSSION
CE is mainly indicated for the evaluation of small bowel diseases, particularly for the diagnosis of obscure GI bleed. CE can be used in a variety of conditions including Crohn’s disease (CD), malabsorption, chronic diarrhea, and evaluation of refractory iron deficiency anemia, abdominal pain, polyposis syndromes, celiac disease and detection of small bowel tumors [5]. Graft versus host disease is a rare additional indication.
CE has been contraindicated in patients with known small-bowel obstruction, strictures, extensive CD, swallowing disorders, pseudo obstruction, motility disorders, cardiac pacemakers and defibrillators.
The main complicaton of CE is capsular retention. Other complications are aspiration, hemorrhage, small bowel obstruction and small bowel perforation [6].
Capsule retention was defined by the International Conference on Capsule Endoscopy (ICCE) in 2005 as the presence of a capsule in the digestive tract for at least 2 weeks or requiring directed medical, endoscopic or surgical intervention [7].
The most frequently reported complication of CE is retention or non-passage. The capsule typically passes within 72 h of administration. The retention rate appears to be between 0.75 and 3% but may be higher in patients with CD.
Retention of capsule endoscope mainly occurs in cases with obscure gastrointestinal bleeding, CD and neoplastic lesions. Other causes of retention were non-steroidal anti-inflammatory drug-induced enteropathy, postoperative stenosis, adhesions, tuberculosis, ischemia and radiation enteritis.
Retention of the capsule is usually asymptomatic, but sometimes causes partial bowel obstruction. Capsule retention indicates the presence of underlying pathology and thus helps in identifying the etiology and site of obstruction [8].
Usually, retained capsules can be extracted with surgery or enteroscopy. Endoscopic retrieval and extraction by push-and-pull enteroscopy using the double-balloon technique have been reported, but subsequent surgical retrieval is often required because of the underlying pathology that caused the stricture or obstruction. Studies suggest that the majority of patients eventually require surgical retrieval.
Laparoscopic surgery is best option for such patients as it carries advantages of minimal invasive surgery and option for curative procedures [9]. Successful outcomes can be expected in patients with retained capsules if the principles of safe laparoscopic surgery, including stringent patient selection, are followed.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}