





Abstract
Tension pneumoperitoneum is commonly caused by gastrointestinal perforation and pulmonary causes are extremely rare. We present a case of a 47-year-old male post motor vehicle accident with a suspected left-sided haemopneumothorax on initial chest x-ray. CT of the chest post chest tube insertion showed a left-sided diaphragmatic rupture and an extensive diaphragmatic hernia. While en-route to the operating theatre, the intubated patient developed tension pneumoperitoneum with positive pressure ventilation and required immediate surgical intervention and repair. A review of the literature around tension pneumoperitoneum and diaphragmatic hernia in trauma is discussed.
INTRODUCTION
Tension pneumoperitoneum is a rare complication in which intra-peritoneal gas, under pressure, causes haemodynamic and ventilatory compromise, necessitating urgent intervention. Gastrointestinal perforation is a much more common cause of tension pneumoperitoneum than pulmonary causes [1]. Tension pneumoperitoneum from trauma involving a lung laceration and co-existing diaphragmatic rupture is extremely rare. In such unstable patients, timely diagnosis and surgical management is required. We describe this rare complication from trauma in our case report, highlighting the challenge in diagnosis, reviewing underlying mechanisms and diagnostic and management options.
CASE
A 47-year-old male was brought to the Emergency department by ambulance after a high speed motor vehicle accident. On arrival, he had a Glasgow Coma Scale of 13, a patent airway with cervical spine collar in situ, spontaneous tachypnoeic breathing with an oxygen saturation of 97% on 15 l of oxygen. He had unequal breath sounds with decreased air entry on the left. He was tachycardic with a blood pressure of 110/70 mmHg. There were multiple bruises and abrasions to his torso and bilateral lower limbs. He had no previous medical history and was otherwise healthy. Initial chest x-ray was suspicious for a left-sided haemopneumothorax (Fig. 1) and an intercostal chest tube (ICCT) was inserted to the left side with a repeat x-ray confirming its position. However, there was minimal drain output and little swing. Subsequent computed tomography (CT) scan of the chest detected a left diaphragm rupture with a large diaphragmatic hernia where most of the left thorax was replaced by intra-abdominal contents (Fig. 2). A decision was made for emergency laparotomy to repair the diaphragmatic hernia. The patient was intubated in the emergency department prior to transfer to the operating theatre. While no ventilation problems were noted during transfer, the patient’s abdomen was seen to become progressively more distended to a point where it became tight and tympanic on percussion (Fig. 3). An underlying lung injury was suspected and the cardiothoracic team was called. At laparotomy, a significant pneumoperitoneum was confirmed with sudden escape of air upon entering the peritoneal cavity. The large hernia containing spleen, stomach and small bowel was reduced and the posterolateral diaphragmatic defect was repaired with a non-absorbable suture. This was followed by a left thoracotomy that identified a superficial laceration in the left upper lobe of the lung which was repaired with Prolene sutures and re-enforced with tissue glue. The patient was then transferred to the intensive care unit in a stable condition and made a good recovery. It is likely that the lung injury was caused secondary to intercostal catheter insertion during resuscitation in the Emergency Department. However, it could also have been secondary to associated left rib fractures or blunt trauma during the accident.
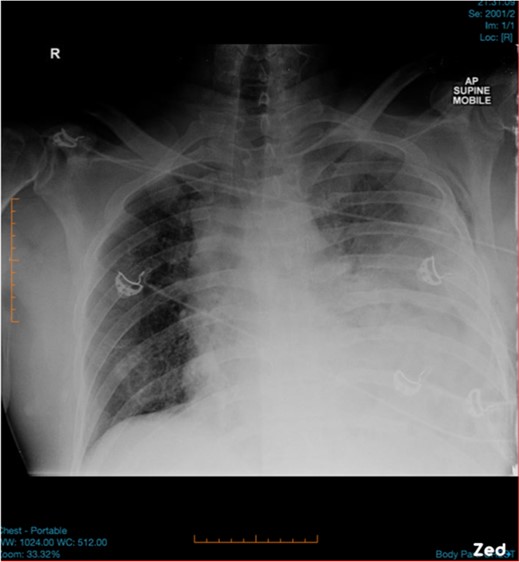
Initial chest x-ray was suspicious for left-sided haemopneumothorax.
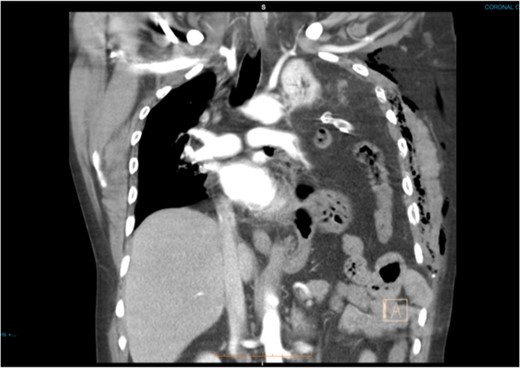
Coronal CT slide showing the entire left haemithorax being replaced by abdominal contents. Note the subcutaneous emphysema post ICCT insertion.

Pre-operative picture showing tension pneumoperitoneum with a very distended abdomen.
DISCUSSION
Tension pneumoperitoneum initially presents with a tympanic abdomen and gross distension, with or without abdominal pain depending on underlying pathology [1]. The clinical picture can be easily confused with intra-abdominal haemorrhage and timely diagnosis is required before circulatory collapse. While chest and abdominal x-rays and focused abdominal sonography for trauma (FAST) are often quick and easy to perform, abdominal CT scan is more specific and sensitive in determining etiology and extent of injury [2].
In this case tension pneumoperitoneum became evident in this patient once mechanical ventilation was commenced. Under normal physiological conditions, intra-abdominal pressure exceeds intra-thoracic pressure by ~20–30 cm of water, therefore, tension pneumoperitoneum should not occur in a simple pneumothorax [1]. In the presence of diaphragmatic rupture, positive pressure ventilation enables this to occur by actively pumping air into this combined thoraco-abdominal cavity.
In most tension pneumoperitoneums, urgent needle paracentesis or insertion of a drain tube is recommended. However, in this case, explorative laparotomy was warranted so that abdominal injury could be excluded and diaphragmatic repair performed.
Traumatic diaphragmatic rupture is uncommon with left-sided injuries more frequently reported than the right due to the protective nature of the liver [3]. Early diagnosis is a clinical challenge as findings from chest x-rays can mimic haemo- or pneumothorax [4], such as in this patient. The inconsistent chest tube output suggested a more complicated injury. If the chest tube drains gastrointestinal contents, then diaphragmatic hernia and complications such as stomach or bowel rupture is indicated [5]. CT of the chest and abdomen has a better sensitivity and specificity and should be performed in haemodynamically stable patients [4].
Due to its mechanism, patients with traumatic diaphragmatic rupture often have injuries that can lead to significant cardiopulmonary impairment. Rib fractures and lacerations of the lung are common, causing haemopneumothorax that may result in tension and mediastinal shift. ICCT may not relieve respiratory distress but may increase the risk of iatrogenic injury to the herniated viscus or the underlying lung [5].
Definitive surgical repair is warranted in all cases of traumatic diaphragmatic rupture even in small defects due to lack of spontaneous healing [4, 6, 7]. While one could argue the possibility of repair via laparoscopy and thoracoscopy, the clinical condition of this patient made it indispensable for open repair.
Management goals of trauma patients are to first stabilize and treat life-threatening conditions, followed by definitive repair of injury. This is often challenging as assessment and diagnosis can be uncertain in a limited timeframe. This is represented here by the delayed recognition of left-sided diaphragmatic rupture that subsequently contributed to the development of tension pneumoperitoneum. Diagnosis in trauma is based on clinical suspicion with radiological support. Prompt surgical management is required to prevent Cadverse outcomes.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}