





Abstract
Tumor involvement of the inferior vena cava (IVC) by hepatobiliary, pancreatic or duodenal malignancies can compromise adequate resection. However, radical resection with negative histological margins remains the only chance of cure. Various techniques are used for venous reconstruction, using a prosthetic graft interposition in most of the cases. However, in case of associated digestive resections, such as pancreaticoduodenectomy, postoperative complications can be responsible for prosthesis infection and related vascular complications. In this setting, the use of biological material for venous reconstruction appears to be preferable. We present an original, easy and useful technique of a venous autoplasty after pancreaticoduodenectomy for tumors involving the anterior wall of the infrarenal IVC, using a patch from the posterior wall of the IVC.
INTRODUCTION
Although rare, tumor involvement of the inferior vena cava (IVC) by hepatobiliary, pancreatic or duodenal malignancies can be difficult to assess preoperatively, and can compromise an adequate oncological resection, especially when found incidentally at laparotomy. However, radical resection with negative histological margins remains the only chance of cure, especially for duodenal tumors which have better prognosis.
Lessons learned from liver transplantation have improved technical considerations and popularized partial or complete resection of the IVC, with acceptable morbidity. Various techniques are used for venous reconstruction, using a prosthetic graft interposition in most of the cases. However, in case of associated digestive resections, postoperative complications can be responsible for prosthesis infection and related vascular complications. In this setting, the use of biological material for venous reconstruction appears to be preferable.
We present an original technique of a venous autoplasty in a woman who underwent pancreaticoduodenectomy for a duodenal adenocarcinoma involving the anterior part of the infrarenal IVC.
CASE REPORT

Preoperative CT-scan showing a huge duodenal mass (*) of 7 cm in size developed from the second part of the duodenum, close to the anterior wall of the infrarenal IVC (**).
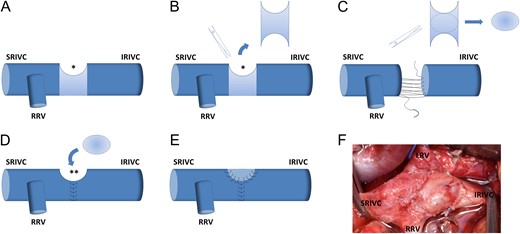
(A) We performed a pancreaticoduodenectomy with en-bloc resection of a 3 cm² area of the anterior wall of the IVC (*). Direct suture of the IVC was not possible and venous reconstruction required the interposition of a graft. (B) Since the posterior wall of the IVC is usually more floppy than the anterior one because of its longer distance from the renal veins, we harvested a transversal patch of 20 × 30 mm in size from the posterior wall of the IVC, below the confluence with the renal veins. (C) Reconstruction of the posterior wall of the IVC was achieved by a direct hand-sewn hemi-circumferential anastomosis using a single-layer non-absorbable 4/0 polypropylene. (D and E) The transversal venous patch was placed longitudinally on the resected area at the anterior wall of the IVC (**), and was sutured using a single-layer non-absorbable 4/0 polypropylene. (F) Intraoperative view showing the venous autoplasty of the IVC. SRIVC, suprarenal inferior vena cava; IRIVC, infrarenal inferior vena cava; RRV, right renal vein; LRV, left renal vein.
The patient received a prophylactic anticoagulation. Postoperative course was marked by a bile leakage on postoperative day 2 which required surgery to repair the hepaticojejunal anastomosis. Postoperative CT-scan showed good permeability of the IVC with no symptoms related to the reconstruction. She was discharged on postoperative day 39.
Pathological examination confirmed the R0 resection of a T4 N1 M0 duodenal adenocarcinoma involving the IVC. She received a 6 months adjuvant FOLFOX chemotherapy regimen and was followed up every 3 months with no recurrence at time.
DISCUSSION
Resection of the IVC is widely performed during surgery for various abdominal and retroperitoneal malignancies, since a radical resection is the only chance of cure. Suprarenal IVC resection without venous replacement has been proposed because the venous collateral pathways can supply the caval flow through the lumbar and epigastric pathways, the renal veins, and the vertebral venous system, which are often well developed in case of a IVC chronic occlusion [1]. However, large dissection of a retroperitoneal tumor and/or thoracoabdominal incisions can both interrupt the ascending collateral venous pathways, resulting in a high risk of major venous insufficiency [2]. In these cases, reconstruction of the IVC is mandatory and can be performed through a direct end-to-end anastomosis, or after the interposition of a venous/prosthetic patch. Nardo et al. [3] reported that resection ≤2 cm of the IVC could be reconstructed by a direct suture while resection >2 cm required the interposition of a graft. In the same way, Tsuji et al. [4] performed a direct suture when the wall defect was less than one-third of the circumference of the IVC. In our case, the venous resection was too large to perform a direct suture of the IVC, either longitudinal or transversal. Therefore, the technique of choice regarding this large venous defect appeared to be a prosthetic reconstruction. However, considering the high risk of infectious complications after duodenopancreatectomy, especially when performed in the settings of a duodenal tumor with a soft pancreatic gland texture and without dilatation of both the pancreatic and the main bile duct, we chose a reconstruction technique that required a large venous patch. Thus, we decided to harvest the posterior wall of the IVC because it was very floppy, that allowed its direct suture. Indeed, these elastic properties of the IVC have already been investigated. Wigmore et al. [5] reported the possibility to easily harvest a venous patch from the anterior wall of the IVC, above the confluence of the renal veins, with a low risk to narrow the IVC because its diameter is larger at this point. Other large veins, such as the portal vein, can also be resected. Our original technique of venous autoplasty could be thus extrapolated to these veins, in order to prevent the use of prosthetic patches and to facilitate reconstruction.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}