





Abstract
Malignant mesothelioma is an uncommon, highly invasive tumor derived from the mesothelial cells of pleura or peritoneum characterized by poor outcome. Mesothelioma was thought to metastasize locally only via direct invasion and not have distant spread. Distant metastases were discovered mostly on post-mortem examination. The authors present a case of 62-year-old man with pleural mesothelioma and brain metastasis.
INTRODUCTION
The authors report a unique case of malignant mesothelioma with distant metastasis to the brain. Pleural mesothelioma was thought to spread directly to local structures with distant metastasis found only on autopsy. The authors present this case to demonstrate that mesothelioma can have distant metastasis and that surgery can improve both survival and quality of life.
CASE REPORT
We report a case of a 62-year-old gentleman who presented with shortness of breath and right-sided chest pain over the period of 12 months. A chest X-ray showed a right pleural plaque that subsequently caused a right pleural effusion (Fig. 1). Decortication, pleurodesis and pleural biopsy were performed with histopathology confirmation of mesothelioma. He declined chemotherapy or radiotherapy, although he was having regular follow-up by the oncologist.

Chest X-ray showing right pleural effusion.
He confirmed being exposed to asbestos, having worked for 20 years in aluminum and margarine factories.
Eighteen months after his initial presentation, he experienced progressive left-sided weakness and left-sided homonymous hemianopia. An MRI scan of his brain showed extra-axial right occipitoparietal enhancing mass (43 × 43 × 47 mm) with surrounding vasogenic oedema. It was isointense to grey matter on T2 and abutting the falx cerebri with midline shift and effacement of the right lateral ventricle (Fig. 2). The lesion was approached through a right occipital craniotomy and entirely removed in a piecemeal fashion. At surgery, it appeared as a greyish-white firm vascular mass with a clear cleavage plane with the surrounding brain. He recovered well after surgery. His left-sided weakness improved significantly with some improvement in the hemianopia. Histopathology revealed metastatic malignant mesothelioma (Fig. 3). The patient had good recovery and was discharged home. On 6-week follow-up, the patient continued to improve with significant improvement in his quality of life.
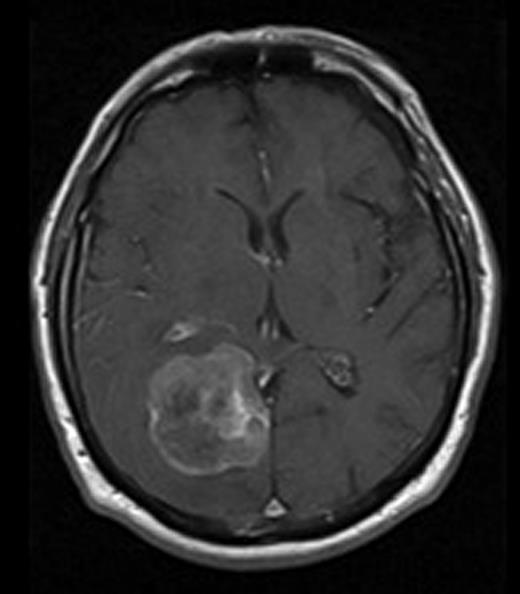
MRI image of brain with gadolinium contrast showing enhancing mass in the right occipital lobe.
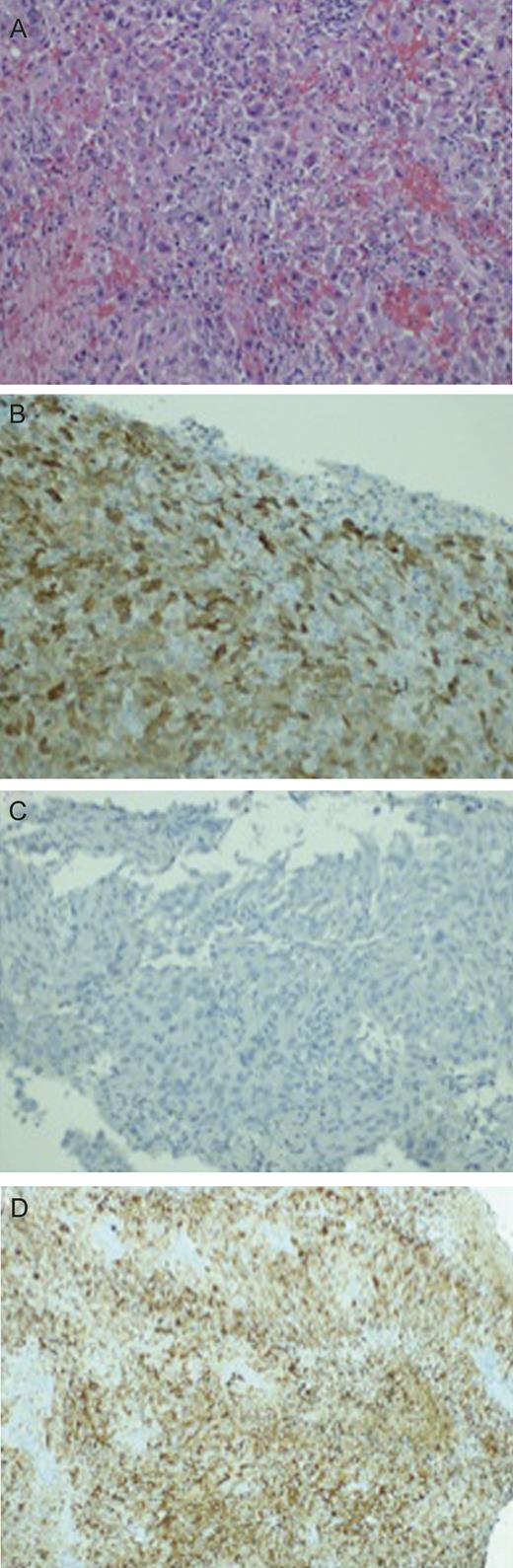
(A) H&E stain of the brain lesion. (B) Positive caltritinin stain. (C) Negative HBME1 stain. (D) Positive C5/6 stain.
Section from the intraoperative specimen showed a large cell-epithelioid malignancy composed of markedly pleomorphic epithelial cells with large hyperchromatic nuclei. Other characteristics included large and multiple nucleoli and abundant acidophilic cytoplasm. Necrosis was also abundant and so were atypical mitoses. Immunohistochemistry is essential to differentiate methastatic mesothelioma from adenocarcinoma. Immunoperioxidase stains demonstrated in fact that the cells expressed vimentin, calretinine, AE1/AE3 and Cam 5.2 as in the previously biopsied pleural lesion. The CK5/6 marker that was previously only lightly positive was now well expressed. EMA and thrombomodulin were also moderately positive. Important negative markers included CEA, CDI5, S100 and TTR-1.
DISCUSSION
Histologically mesotheliomas may be purely epithelioid (50%) or of mixed histology (30%). Pure sarcomatous types are seldom seen as diffuse neoplasms.
Malignant mesothelioma is an uncommon tumor that arises from the serosal surfaces. More than 80% of tumors arise from the pleura; however, primary mesothelioma of the peritoneum, pericardium and tunica vaginalis have also been reported [1]. Wenger et al. first reported the association between mesothelioma and asbestos exposure [2].
The risk of developing mesothelioma after asbestos exposure is ∼8%, depending on the duration and intensity of exposure [3].
Malignant pleural mesothelioma usually presents between the fifth and seventh decade of life and can be difficult to diagnose due to the vagueness of the presenting symptoms including dyspnea and nonpleuritic chest pain [4]. The median survival is only ∼9months from diagnosis with death usually due to thoracic disease [5]. This rapid progression may have contributed to the belief that mesothelioma rarely has distant metastasis. Falconieri et al. [6] reviewed 171 cases of malignant mesothelioma at autopsy and discovered that over 54% of patients had distant metastases. The sites most commonly affected were the liver, adrenal glands and kidneys (56, 31 and 30%, respectively). Cerebral metastasis was found in only 3%. Wronski and Burt [7] also reviewed the post-mortem findings and they concluded that the incidence of distant metastasis from pleural mesothelioma is around 50% and the incidence of cerebral metastasis around 5–10%.
Although there are numerous reported cases of cerebral metastasis from malignant pleural mesothelioma, the majority of cases were post-mortem findings. Furthermore, only eight patients had neurological manifestation of cerebral disease at the time of diagnosis [3, 6, 8]. The case we report is interesting for the presentation of the intracranial pathology 18months after the initial presentation, well beyond the reported median survival for this lesion. The good postoperative neurological recovery also emphasizes the role of surgery to extend survival in the presence of locally controlled primary disease. To the best of our knowledge, this case represents the third report of symptomatic cerebral metastases from malignant mesothelioma that was treated by surgical excision via craniotomy, where ante-mortem histological diagnosis was obtained.
With an increasing incidence of mesothelioma, the treatments available are also expanding. In the past, single-modality therapy alone (surgery, radiotherapy and chemotherapy) has failed to improve survival significantly. Multi-modality approaches are producing favorable results [8]. Furthermore, several new therapeutic techniques, such as photodynamic therapy, immunotherapy and intracavitary chemotherapy, are increasing survival and retarding disease progression.
We present this case to demonstrate that metastatic mesothelioma can have distant metastasis to the brain. As a direct result of improvements in treatment, the survival of patients with malignant mesothelioma will continue to improve, and more patients are likely to present with metastatic disease. It is, therefore, important to recognize the metastatic potential of mesothelioma. As we have demonstrated in this case, surgical excision of cerebral metastases can provide symptomatic relief, and surgical treatment may therefore be justified in enhancing the patient's quality of life.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}