





Abstract
We report the case of a 59-year-old obese female who developed an abdominal wall haematoma during administration of prophylactic clexane. Compared with the non-obese, the subcutaneous tissue of the obese is considered dysfunctional and has a different vascular structure and extra-cellular matrix composition. While the development of an abdominal wall haematoma is relatively uncommon, when they occur they can have fatal consequences. The altered subcutaneous tissue environment in the obese attenuates the normal external compression of an abdominal wall haematoma and as a result the obese are at greater risk of haemorrhage.
INTRODUCTION
Haematomas of the superficial abdominal wall occur infrequently in the hospital setting. Though uncommon the well-described complications of an abdominal wall haematoma include uncontrolled haemorrhage requiring blood product transfusion and death [1]. A number of factors are known to predispose to the development of an abdominal wall haematoma. These include older age, female sex and the use of anti-platelet or anti-coagulant agents [2].
Obesity is an additional factor that may complicate the formation of an abdominal wall haematoma. Compared with the non-obese, the sub-cutaneous tissue of the obese is considered dysfunctional and has a different vascular structure and extra-cellular matrix composition. The self tamponade effect that limits the extension of an abdominal wall haematoma may be deficient in the obese. Here we report the case of a 59-year-old obese female who developed an abdominal wall haematoma and haemodynamic instability during admission in our hospital.
CASE REPORT
A 59-year-old obese female was admitted to the hospital with fever on the background of poorly controlled Type 2 diabetes (Hba1c 9.5%). The patient's background included ischaemic heart disease, chronic kidney disease, peripheral vascular disease and a right-side, below-knee amputation. On examination, the patient's weight was 125 kg, height 154 cm and body mass index was 53. A diabetic foot ulcer was identified at the base of the left heel.
Two weeks later, the patient remained hospitalized for the management of an infected diabetic foot ulcer and awoke one morning with acute abdominal pain and shortness of breath. The patient was haemodynamically compromised with a pulse rate of 120 and blood pressure 90/60 lying. The haemoglobin fell overnight from 126 to 90 g/l and a few hours later there was a further fall to 79 g/l. The medical emergency team were called. Platelet count was 242, international normalized ratio (INR) 1.0, activated partial thromboplastin time (APTT) 33 and anti-factor Xa level 0.41 in keeping with prophylactic clexane administration. A CT scan was performed, which demonstrated a large abdominal wall haematoma (see Fig. 1).
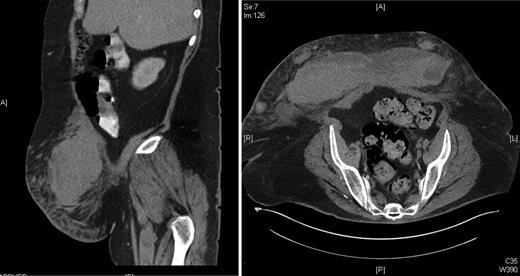
CT abdomen of a 59-year-old obese female with an abdominal wall haematoma.
DISCUSSION
There are limited data on the relationship between weight or body mass index (BMI) and the development of an abdominal wall haematoma [3]. In the case series we reviewed, the weight or BMI of the patient is rarely mentioned. Yet, where a photographic image is published, the patient's weight and abdominal girth often appear excessive [4].
It has been recognized that women are more prone to haematoma formation owing to the relative lack of abdominal wall muscle mass compared with men. The effects of pregnancy are also known to contribute to haematoma formation. Despite a paucity of evidence, it has been suggested that the obese are at risk of developing complicated abdominal wall haematomas and the presence of increased abdominal fat may predispose to an increased risk of haemorrhage [5].
The adipose tissue of the obese differs from those with a normal BMI and obesity-associated adipose tissue dysfunction is an entity thought to be caused by a combination of inappropriate angiogenesis, localized inflammatory reaction and hypoxia [6].
Specifically, the vascularity of subcutaneous tissue in the obese is abnormal when compared with controls [7]. There is an increase in the number and size of blood vessels in the abdominal wall and there are structural alterations in the small arteries. These processes are driven by an increase in local vascular endothelial growth factors and angiopoietins [8].
Change in the subcutaneous tissue of the obese is not limited to the vasculature and there are differences in the extra-cellular matrix when compared with the non-obese with the structure of both elastin and collagen affected. Quantification of elastin in one trial showed that adipose tissue from obese individuals had <6% total elastin content compared with ∼12% in lean individuals [9].
As in the elderly where vascular fragility and changes to the subcutaneous tissue environment limit the external compression of an abdominal wall haematoma, the same may be said of the obese. For this reason the tamponade effect that contributes to the cessation of haemorrhage may be attenuated in obese patients [10].
To summarize, although abdominal wall haematomas are not common, they are potentially fatal. The literature makes little reference to the weight or body mass index of this group of patients. It has been shown that there are changes in the vascularity and the extra-cellular matrix in the subcutaneous tissue of the obese. It is thought that the lack of external compression of an abdominal wall haematoma makes bleeding more likely. For this reason, the obese appear at greater risk from this relatively uncommon phenomenon and vigilance is required in this group of patients to ensure their haemodynamic stability and safety.

{kind=link}