





Abstract
Thoracoliths are rare benign intrapleural fibrotic structures with a necrotic fat core. There are 19 previous reported cases in the literature. This case report presents for the first time, a patient with two thoracoliths within the same hemithorax. Both lesions were identified incidentally in the left hemithorax by computed tomography and remained in the same position on repeat imaging. The lesions were removed by a video-assisted thoracic surgery approach. Histology revealed a 20mm and a 14mm lesion, with a fibrotic dense collagen shell surrounding a non-viable necrotic fat core. This case demonstrates that thoracolithiasis is a rare differential diagnosis for incidental multiple non-mobile lesions within the thorax.
INTRODUCTION
Thoracolithiasis was first described in 1968 by Dias (1). A thoracolith is an intrapleural benign fibrotic structure with a necrotic fat core also described as a pleural stone, intrathoracic calculus or pleurolith (2). The aetiology is unknown and previous authors have described no history of previous trauma, intervention, or pleurisy in patients with these lesions (3).
A search of the literature finds 19 previous cases of surgically removed thoracoliths (1-8) and 12 radiologically diagnosed thoracoliths (9,10), all of which have been lone nodules. This paper reports for the first time two separate and discrete thoracoliths within the same hemithorax.
CASE REPORT
A 71 year old male Caucasian teacher was incidentally found on Computed Tomography (CT) of the colon to have two well-defined nodules in the left hemithorax. There was no other abnormality within the thorax or abdomen. He was a non-smoker, with only minimal exposure to a classroom with an asbestos roof. He had no history of chest trauma, intervention or pleurisy. A further high resolution CT scan of the chest demonstrated a well-defined rounded 11mm nodule arising from the pleura of the left diaphragmatic surface (Figures 1a and b). A larger 15mm rounded soft tissue lesion containing calcification was noted in the pleura of the left paravertebral region adjacent to the lower lobe (Figure 2). No other abnormality was present in the chest. The multidisciplinary decision at that time was to monitor with an interval high resolution CT scan of the thorax. Four months later the scan showed a slight increase in size of both nodules and a decision with the patient and by a multidisciplinary meeting was to resect the nodules for diagnosis. At this stage the nodules were in the same position as on the initial scan.
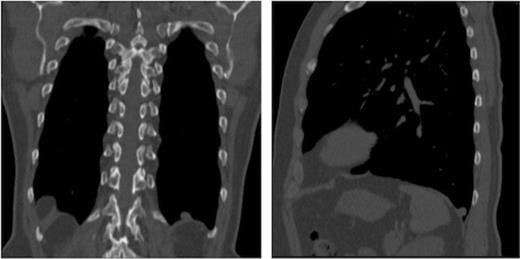
Coronal CT image of the thorax demonstrating nodule 1 overlying the left hemidiaphragm. Sagittal CT image of the left hemithorax demonstrating nodule 1 overlying the left hemidiaphragm
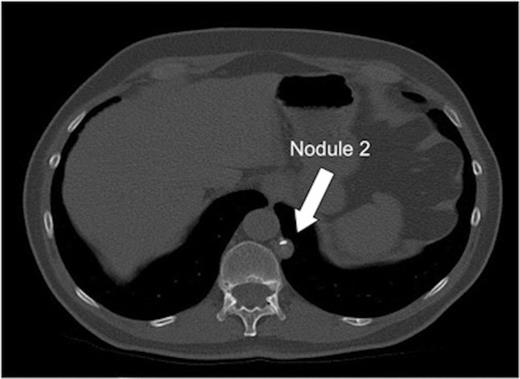
Transverse CT image of the thorax demonstrating nodule 2 adjacent to the mediastinum, vertebral body and descending aorta
He underwent a left single port video-assisted thoracoscopy. With the lung deflated it was possible to see two free and mobile white spherical masses within the left hemithorax. These were removed from the intrapleural space with no dissection required. They were sent for histopathological examination.
Macroscopically, the two white nodules had a smooth outer surface, measuring 14 x 10 x 8mm and 20 x 18 x 15mm (Figure 3). The larger one had a small nubbin protruding from the surface measuring approximately 2mm. No stalk was seen on either specimen. On slicing, the smaller nodule consisted almost entirely of soft rubbery white tissue, similar to cartilage, with a small area of brown discolouration centrally. The larger fragment had a similar pale shell of tissue measuring 3-4mm in thickness and within the centre there was soft and focally gritty material that had a brown/yellow mottled appearance, with focal calcification (Figure 4a).

Both nodules after retrieval from the left hemithorax
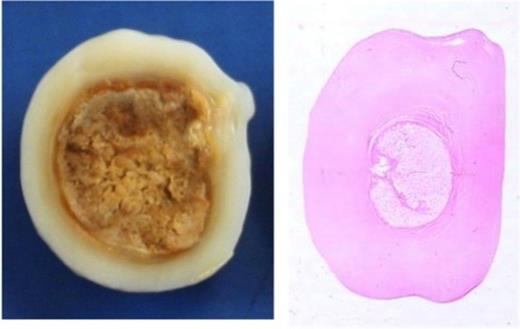
Cut section of the smaller nodule showing a thick, pale shell of tissue with appearances similar to cartilage. H&E stained whole-mount section (1x magnification) of the same slice of tissue
Microscopically, both nodules showed similar histological features. The larger nodule required prolonged, gentle decalcification before reasonable tissue sections could be obtained. Each had a thick shell of dense paucicellular collagen arranged as concentric layers with only a few fibroblasts and inflammatory cells present peripherally (Figures 4b and 5). The shell was devoid of cartilage and it encased necrotic adipose tissue (Figure 6) in which there was focal dystrophic calcification. No granulomatous inflammation, lung parenchyma, abscess formation, caseous type necrosis or neoplasm was identified.
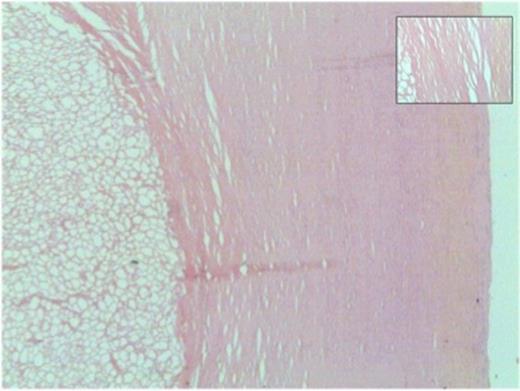
Thick shell of paucicellular collagen surrounding necrotic fat (40x magnification). Inset: Closer view of concentrically arranged thin layers of collagen
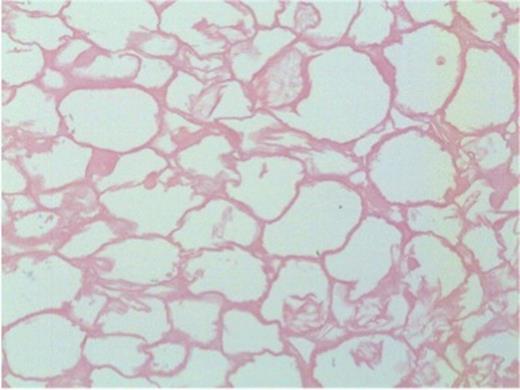
Necrotic adipose tissue centrally within the nodule (200x magnification)
DISCUSSION
Thoracolithiasis is an uncommon benign abnormality. As imaging is more widely available further cases of thoracolith incidentalomas will be diagnosed. It is now clear that multiple thoracoliths may be found and, while uncommon, it is a differential diagnosis for the incidental lung nodule. In this case there was no change in position of the nodules between the two scans, a finding that has previously been used to diagnose pleural pearls (9,10). Further work needs to be done to understand the aetiology of these uncommon nodules. This case demonstrates that thoracolithiasis is a rare differential diagnosis for incidental multiple non-mobile lesions within the thorax.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}