





Abstract
We highlight the case of a double Inferior Vena Cava (IVC) encountered in a multi-visceral recovery operation on a deceased donor. In such cases pre-operative abdominal cross sectional imaging is usually not available hence the procurement surgeon needs to rely on vigilance and awareness of other potential anatomical variations that are associated with the condition. We outline our operative approach, summarize the embryological development of IVC and present the case as a reminder of this rare anatomical variation.
INTRODUCTION
The safe, effective recovery of organs with maximal transplant potential is of paramount importance particularly, in the context of acute shortage of donor organs. Vascular anomalies at the time of operation can present significant challenges testing the technical and anatomical knowledge of the recovery surgeon. We highlight the case of a double Inferior Vena Cava (IVC) encountered in a multi-visceral recovery operation, outline our operative approach and serve as a reminder of this rare anatomical variation.
CASE REPORT
The donor was a 34-year-old brainstem dead male who had suffered a non-traumatic intracranial haemorrhage. There was no significant past medical history including any congenital defects. No previous or current abdominal cross sectional imaging had previously been under taken. Abdominal and thoracic multi organ procurements were planned with heart, lungs, liver, kidneys and pancreas accepted for transplantation.
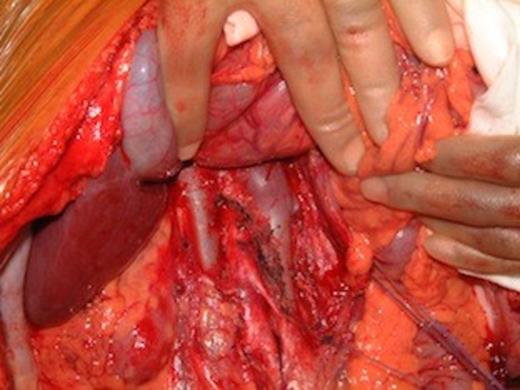
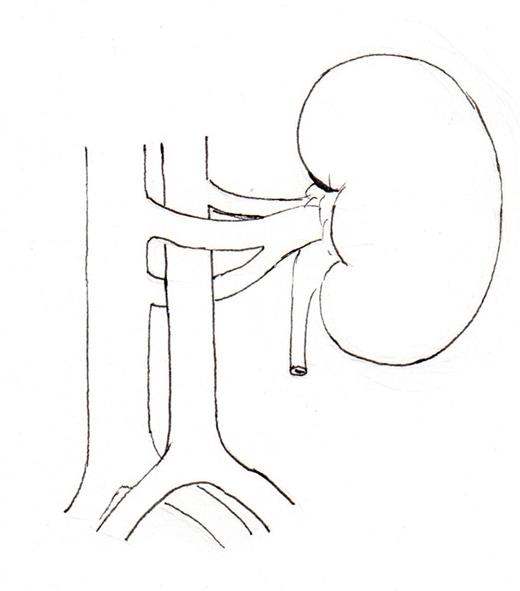
Intra-operative photograph of double IVC in a deceased multi organ donor
Laparotomy revealed the presence of a double IVC (Figure 1). The two vena cava were approximately of equal caliber. At the level of the kidney, the left renal vein joined the left vena cava which then passed to the right and joined the right vena cava. The combined IVC trunk then traversed the normal retro hepatic route before passing through the diaphragm in to the right atrium in normal anatomical position. Both kidneys were of normal size with both the ureters located in normal positions. Liver also had a normal anatomy including vascular inflow and venous drainage. No other anatomical anomalies were encountered. Standard multi organ retrieval protocols were followed. Thoracic organs (heart and lungs) were procured first and no anatomical anomaly was reported. The supradiaphragmatic IVC was incised after start of aortic perfusion to ensure adequate flush of both right and left IVC. Liver was removed after dividing supra and common infra hepatic IVC, portal vein and celiac trunk. The left renal vein was retrieved with the intact left IVC which was divided before its junction with the right IVC. Similarly the right renal vein was retrieved with intact right IVC. Implantation of the liver and both kidneys were standard and without any complications
DISCUSSION
Duplication of the IVC is one of the most common anomalies affecting the inferior vena cava (IVC), next to transposition (left sided), and has been reported to occur in 0.2-3% of the population (3). Recognizing this anomaly is important in order to procure abdominal organs safely and also to recognize other anomalies that may co-exist with this condition. Duplication of IVC in the context of organ procurement has not been previously described in literature.
During the embryonic development the formation of the IVC is a complex multistep process involving three paired venous channels (posterior cardinals, sub cardinals and supra-cardinals). The adult IVC is the result of, the formation of communicating channels between them and the eventual regression of specific segments before the 8th week of gestation (1), (2). Duplication of IVC arises as a result of the persistence of the right and left supra cardinal and sub cardinal veins (2). The right vena cava is usually dominant. The left vena cava joins it in front or behind the aorta at the level of or just above the left renal vein (Figure 2a, b, c, d). The size of the left vena cava can vary significantly and drain directly into the left renal vein (4). Associated conditions of relevance to the abdominal procurement surgeon include anomalies of the renal veins (circum aortic renal collar, and retro aortic renal vein) (1), right retro caval ureter (3), horseshoe kidney, congenital right renal agenesis (4) and cloacal exstrophy (5). Lumbar vein aberrations, including agenesis and collaterals have also been associated with vena cava anomalies.
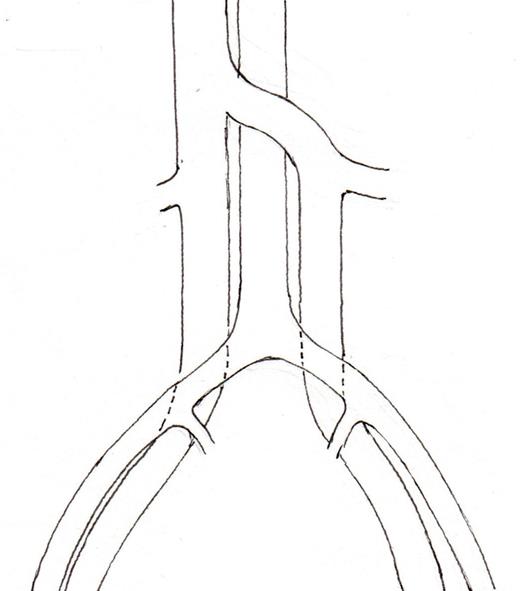
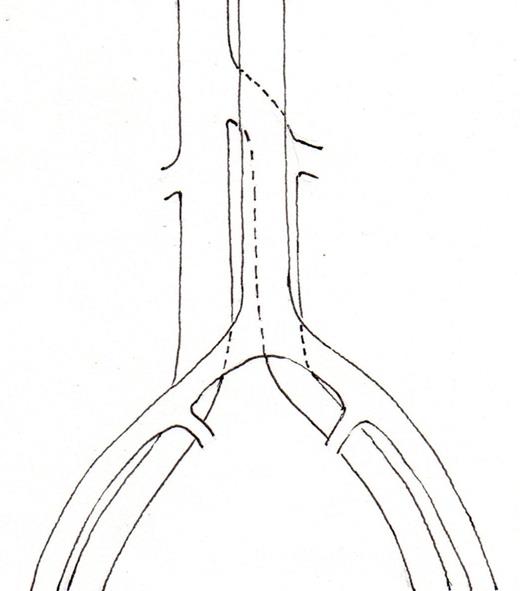
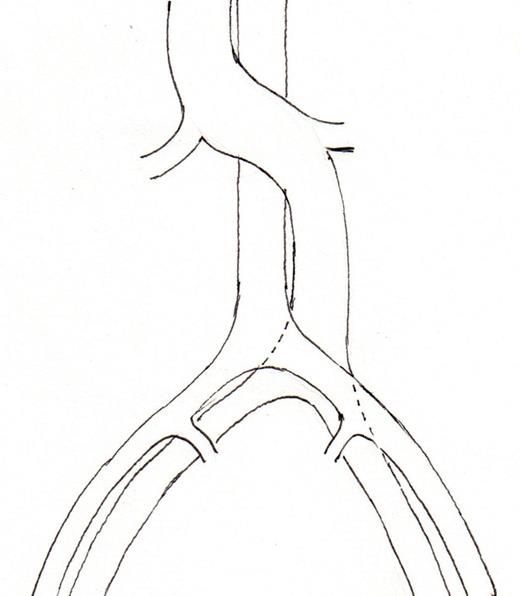
Schematic representation of common disposition of double IVC. (2a) common variant, left IVC crossing in front of the aorta, (2b) The left IVC passes behind the aorta, (2c) Transposition of IVC (left IVC), (2d) circum aortic left renal vein.
A computerized tomogram (CT) or a magnetic resonance (MR) angiogram arethe best diagnostic modalities for identifying and mapping venous anomalies within the retro peritoneum. If preoperatively identified, this will allow for safe surgical planning and outcomes (6). Whilst, a rare condition one should be alert to potential caval abnormalities when reviewing abdominal imaging of potential donors, (Figure 3) as anomalous venous structures tend to be dilated and tortuous making injury more likely (7). In deceased donor procurement setting, cross sectional imaging is usually not available at and a surgeon will have to rely on vigilance, awareness of potential anatomical variation and ensure adequate exposure of major vessels. The identification of a duplicated IVC in our donor did increase operative time, in order to define the true nature and extent of the anomaly and to plan the procurement of intra abdominal organs without compromising the utilization of procured organs for transplantation.

{kind=link}
{kind=link}