





Abstract
We present a rare case of an ectopic main right renal artery originating as part of the coeliac axis. Renal arteries are usually paired vessels which originate directly from the aorta to supply each kidney. Variations in their origin and numbers have been reported by many authors. However, there has only been one previous report of a left main renal artery arising from the coeliac axis in the medical literature, in 1980, seen during angiography. We believe we have the first CT angiographic evidence of such anatomy. This important aberrant anatomy must be noted not only for its rarity but also for its implications in the field of transplant surgery and interventional radiology. There will be more similar reports as non-invasive imaging is being used ever more frequently.
INTRODUCTION
Renal arteries are usually paired vessels which originate directly from the aorta to supply each kidney. We present a rare case of an ectopic main right renal artery originating as part of the coeliac axis.
CASE REPORT
A 75 year old lady was referred for a vascular opinion for management of an abdominal aortic aneurysm incidentally noted on MRI when she was being investigated and diagnosed with spondylolisthesis. Her co-morbidities included hypertension, hypothyroidism and hypercholesterolaemia. She had no previous operations and she was a non-smoker. On examination, a pulsatile, non-expansile mass in the epigastrium was the only positive finding.

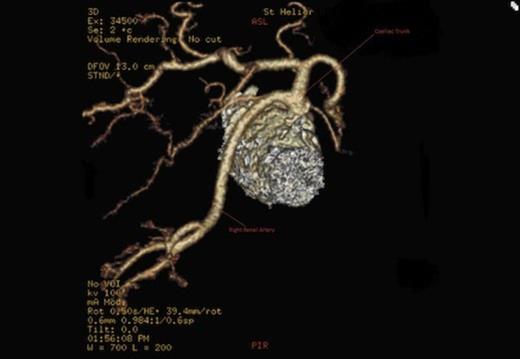
Origin of the right renal artery

Origin of the right renal artery
A CT scan revealed an aneurysmal distal thoracic aorta measuring 40mm and 49mm at the level of the diaphragm and of normal calibre at the left renal artery. The right renal artery very interestingly had its origin from the coeliac axis with no significant renal artery disease and the left renal artery showed calcific disease with post-stenotic dilatation at its ostium from the aorta. There were also no accessory renal vessels noted.
Origin of the right renal artery
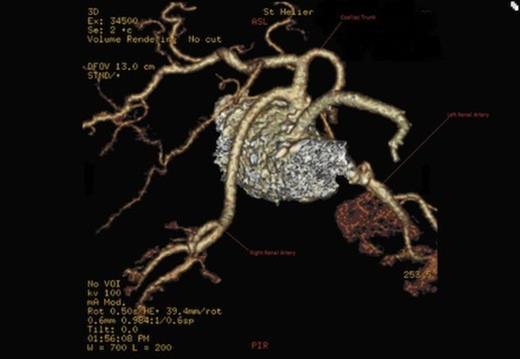
Origin of the right renal artery
DISCUSSION
Anatomic variation of the renal blood supply has been broadly divided into two groups by Garti and Meiraz in 1980 (a) multiple renal arteries originating from the aorta or branches thereof; (b) ectopic origin of a single main renal artery (1).
There are a large number of variants noted in literature. Some of which are noted below:
Schaffer et al (2) noted a renal artery originating off the aorta above the coeliac axis in 1981.
Gillespie et al (3) on the other hand, reported not a main, but an accessory upper pole renal artery arising directly from the coeliac axis as well.
Kruyt (4) reported a single left main renal artery originating from the splenic artery
Dalcik et al (5)reported a single right main renal artery originating together with the superior mesenteric artery from a common trunk from the aorta at L2.
Armstrong et al (6) documented their case of a common origin of the inferior mesenteric artery and left lower pole accessory renal artery in association with a horseshoe kidney and cited previous reports of common origins for the inferior mesenteric artery and renal artery.
Other than our case, Garti and Meiraz (1) have the only other available record of a single main renal artery originating from the coeliac axis. They reported a single left renal artery arising from the coeliac.
Therefore, we have only the second documented single main ectopic renal artery originating directly from the coeliac axis. Furthermore we are the only ones to have CT angiographic evidence of the above.
Our case, together with others which show renal vessels originating from the ventral splanchnic arterial system (eg. coeliac and branches thereof, SMA & IMA) can possibly be explained by the periaortal plexus first described by Bremer (7) in 1915, and by the presence of the sub-peritoneal arterial plexus first described by Sir William Turner (8) in 1863 and more recently highlighted by Shoja et al (9) in 2011.
Shoja’s team has noted that these vessels have been shown to act as a communication between the parietal and visceral branches of the abdominal aorta and possibly be a route for metastatic spread in any direction between the retroperitoneal and pelvic organs and the gastrointestinal system.
These researchers specifically allude to accessory renal arterial supply supplementing a main renal artery or arteries. The accessory vessels could arise or persist from various other named vessels as the kidneys ascend during embryonic growth and other organogenesis concurrently occurs in close proximity.
The accessory vessel could indeed become the main vessel if the original main vessels degenerated for whatever reason. The presence of the peri-aortal and sub-peritoneal arterial connections may have allowed for the coeliac axis, for example, to communicate with the renal vessel and establish a patent vessel, whilst at the same time, for reasons such as extrinsic pressure/blockage or intrinsic arrest of growth, the kidney’s original route of supply from the aorta may have degenerated.
In conclusion, we believe that further research is needed to elucidate the embryological or non-embryological causative factors for such variation in renal anatomy. Whatever the causative factor, we also believe that our case is important not only for its rarity but also for its implications in the field of transplant surgery and interventional radiology.

{kind=link}
{kind=link}
{kind=link}
{kind=link}