





Abstract
Thyroid carcinoma is rare comprising 1% of all malignancies and commonly presents as a neck lump. Papillary thyroid carcinoma unlike follicular thyroid carcinoma tends not to metastasise to distant sites.
We present a case of papillary thyroid carcinoma presenting as a solitary asymptomatic pelvic bone metastases and highlight current management of bone metastases. A 59-year old female was found on abdominal computerised tomography to have an incidental finding of a 4.5 cm soft tissue mass in the right iliac bone. Biopsy of the lesion confirmed metastatic thyroid carcinoma. There was no history of a neck lump, head and neck examination was normal. Further imaging confirmed focal activity in the right lobe of the thyroid. A total thyroidectomy and level VI neck dissection was performed and histology confirmed follicular variant of papillary carcinoma.
Early detection of bone metastases have been shown to improve prognosis and thyroid carcinoma should be considered as a potential primary malignancy.
INTRODUCTION
Thyroid carcinoma comprises 1% of all malignancies but is the commonest malignant endocrine tumour. Annual incidence in the UK is reported at 2.3 per 100,000 women and 0.9 per 100,000 men (1).
Papillary thyroid carcinoma is the most common comprising 80% of all thyroid malignancies. It occurs in all age groups but is most common in the 3rd to 5th decades (2). Whilst, lymph node metastases are often present at diagnosis, haematogenous spread is a rare and late event. In contrast, distant metastases (commonly to bone and lung) are more common in follicular thyroid carcinoma, which represents approximately 10–20% of all thyroid cancers (2).
Distant metastases are noted in 1-3% of patients with thyroid cancer at initial diagnosis whereas 7-23% develop distant metastases during the course of the disease process (3). Commonly, thyroid carcinoma presents as a neck lump (which may be clinically solitary or multinodular) and initial presentation in the form of bone metastases leading to the diagnoses of thyroid carcinoma is rare.
CASE REPORT
A 59-year old Afghani woman presented initially to the acute medical team with a history of hypokalaemia and hypertension. Investigations confirmed non-suppressed hyperaldosteronism and computerised tomography (CT) imaging of the abdomen confirmed adenoma of the left adrenal gland. However, imaging also noted an incidental finding of a soft tissue mass in the right iliac bone measuring 4.5cm transversely (Fig. 1). Initial differentials included plasmacytoma and chondroma.
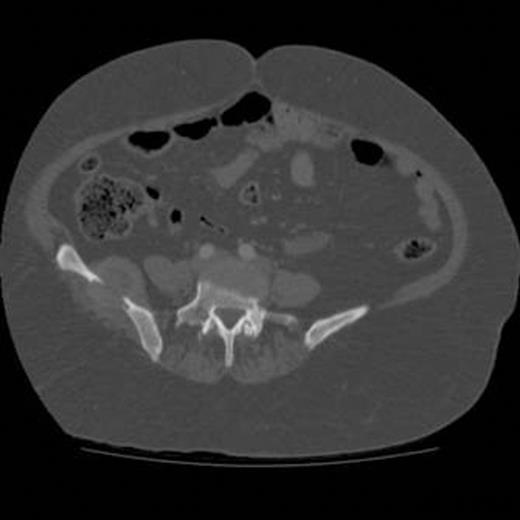
Axial CT image of abdomen demonstrating the mass noted in the right iliac bone of the pelvis measuring 4.5cm transversely.
The patient underwent a biopsy of the right pelvis, which confirmed metastatic follicular type thyroid carcinoma and was urgently referred to the Otolaryngology department. There was no history of a neck lump or associated head and neck symptoms and neck examination was normal. Initial CT of the neck and thorax revealed an area of change in the right lobe of the thyroid gland measuring approximately 2cm. To further define this lesion and rule out other potential bone metastases positron emission tomography- computerised tomography (PET-CT) and Technetium-99m whole body bone scan was arranged. Imaging confirmed focal activity in the right lobe of thyroid, normal neck nodes and a solitary lesion in the right iliac wing with no further distant metastases. A total thyroidectomy and level VI neck dissection was conducted. Within the right lobe of the thyroid a nodule measuring 25mm in diameter was noted on macroscopic appearance (Fig. 2).

Total thyroid specimen with a 2.5cm nodule evident within the right thyroid lobule.
Histology confirmed follicular variant of papillary thyroid carcinoma (FVPTC). Following surgery the patient was referred to Orthopaedics for surgical resection of the solitary right iliac wing bone metastases lesion with radioactive-iodine therapy to follow.
DISCUSSION
Commonly, thyroid carcinoma presents with a solitary or multi-nodular neck mass. The reported incidence of metastases to the skeletal system from thyroid carcinoma ranges from 1% to more than 40%, forming the second most common site following lung involvement (4). The initial presentation of distant metastases (3-4%) in patients with differentiated thyroid carcinoma is a rare event.
Bone metastases from primary tumours of unknown origin are commonly attributed to prostate, breast or lung and in more than 80% of patients, symptoms such as pain, swelling or fracture are evident (5). However, as reflected in the case report, thyroid carcinoma may present with asymptomatic bone metastases and should be considered amongst the potential differential diagnoses. Commonly reported osseous sites include the vertebrae, skull, pelvis and femur (3).
Follicular carcinomas have been reported to show a greater prevalence to metastasise distally than papillary or anaplastic subtypes. However, this may due the generic use of the term follicular carcinoma prior to the more recent recognition of specific sub-types, including FVPTC (4). Although, FVPTC is thought to behave in a similar clinical manner to true papillary thyroid carcinoma, it has been suggested that some specimens of FVPTC may mimic the pathologic features and clinical behaviour of follicular carcinoma (6). Nonetheless, recent studies report a higher relative incidence of papillary carcinoma giving rise to bone metastases (4).
The prognosis is favourable in differentiated thyroid carcinoma with a 10-year survival rate of 80-95% (1) but this is decreased to 50% when distant metastases are present. Furthermore, age at diagnosis of papillary or thyroid carcinoma is a consistent prognostic indicator with the risk of recurrence and death increasing with age, especially in those over 40 years (1).
Bone metastases are associated with a poorer prognosis in comparison to metastases to the lung. In patients with bone metastases, whether isolated or associated with lung metastases, the prognosis is markedly poor with 10-year survival rates reported from 13-21% (7).
Current guidelines advise bone metastases should be treated with a combination of surgery, external beam radiotherapy, and 131Iodine therapy. Improved survival and quality of life has been shown following removal of up to five bone metastases and hence surgical excision is recommended for accessible, solitary, isolated metastases (1).
The late detection of bone metastases may, in part explain the associated poor prognosis. Patients presenting with initial distant metastases compared to those who develop distant metastases after initial presentation seem to have better outcomes in relation to overall survival. (7) Recently the use of 131Iodine scanning to ensure early detection of bone metastases when tumour burden is small has been shown to improve response to 131Iodine therapy.

{kind=link}
{kind=link}