

Abstract
Laparoscopic liver resection is increasingly favored as the standard of care for liver tumors; however, achieving a good surgical field remains challenging if the resection line is in the paracaval portion of caudate lobe. Here, we report a hepatoduodenal ligament lifting technique using the round ligament of the liver to secure the surgical field. As the caudate lobe was excised from the right side, the elongated round ligament of the liver was passed from left to right behind the hepatoduodenal ligament, and the Endoloop ligated to the distal end of the round ligament was pulled and fixed to the left upper abdomen. The caudate lobe was excised from the left side, and the reverse procedure was performed. These techniques facilitate hepatic dissection in this area by applying appropriate tension between the hilar plate and the liver, and the stable exposure of the posterior aspect of the hepatoduodenal ligament.
Introduction
Laparoscopic liver resection has become the standard of care for liver tumors owing to its minimally invasive nature. However, laparoscopic liver resection has movement limitations and the difficulty varies significantly depending on the resection site. Here, we report the use of ‘the hepatoduodenal ligament lifting technique’ with the round ligament of the liver, which represents the remnant umbilical vein to secure the surgical field for resection of the hepatic caudate lobe.
Case presentation and surgical technique
Case 1: A 72-year-old man with a 45 mm hepatocellular carcinoma protruding from the caudate process underwent planned laparoscopic partial hepatic resection S1/6 from the right side of the hepatoduodenal ligament (Fig. 1). The dissection line was posterior to the hepatoduodenal ligament, and securing and stabilizing the surgical field was challenging. The round ligament was transected leaving a sufficient length and passed from left to right behind the hepatoduodenal ligament. The Endoloop (Ethicon, Somerville, NJ, USA) ligated to the distal end of the round ligament was exteriorized through the abdominal wall (Fig. 2a–d). By pulling and fixing the Endoloop to the left upper abdomen using forceps intermittently according to the hemostasis time of Pringle’s maneuver, the operative field of the posterior aspect of the hepatoduodenal ligament was properly secured (usually trapezoidal traction accompanied by Pringle’s maneuver). Appropriate tension was obtained between the hilar plate and resected liver, and laparoscopic partial liver resection S1/6 was completed (Supplementary Video 1).
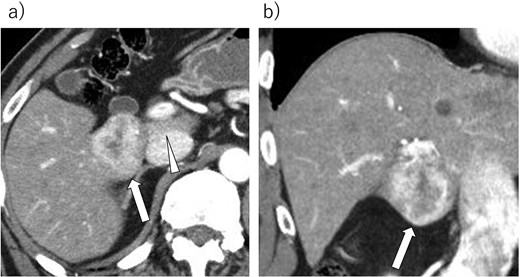
A 45 mm hepatocellular carcinoma of S1 protruding from the caudal process. (a) Axial section. (b) Coronal section. Arrow: Tumor. Arrow head: Resection line.
{kind=link}
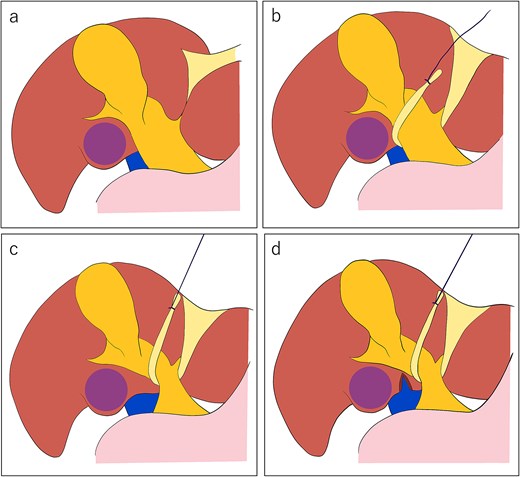
(a) The tumor (solid purple circle) is located in the caudate process, and the dissection line is posterior to the hepatoduodenal ligament. We planned a right-sided approach. (b) The elongated round ligament of the liver is passed from left to right behind the hepatoduodenal ligament, and the Endoloop is ligated the distal end of the round ligament. (c) The Endoloop is pulled to the left upper abdomen through the abdominal wall and fixed by forceps. (d) The hepatic resection underwent a good surgical view and appropriate tension between the hilar plate and resected liver.
{kind=link}
Case 2: A 63-year-old man (body mass index; 31.2 kg/m2) with a 24 mm hepatocellular carcinoma in the Spiegel lobe underwent planned laparoscopic partial hepatic resection of S1 from the left (Fig. 3). The excision line was located posterior to the hepatoduodenal ligament. To secure the surgical field, the elongated round ligament of the liver was passed from right to left behind the hepatoduodenal ligament and pulled to the right upper abdomen using the same procedure as described above (Fig. 4a–d), along with compression of the lateral segment of the liver using a Nathanson retractor (Mediflex Surgical Products, Islandia, NY, USA). Subsequently, the operative field of the posterior aspect of the hepatoduodenal ligament was secured, appropriate tension was obtained between the hilar plate and the resected liver, and laparoscopic partial liver resection S1 was completed (Supplementary Video 2).
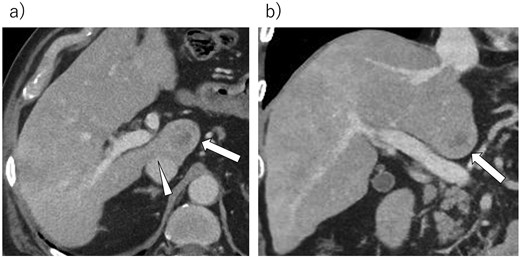
A 24 mm hepatocellular carcinoma of S1 in the Spiegel lobe. (a) Axial section. (b) Coronal section. Arrow: Tumor. Arrow head: Resection line.
{kind=link}
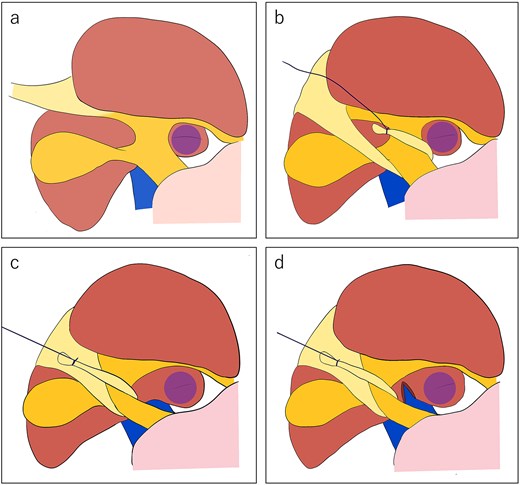
(a) The tumor (solid purple circle) is located in the Spiegel lobe, and the dissection line is poterior to the hepatoduodenal ligament. We plan left-sided approach. (b) The elongated round ligament of the liver is passed from right to left behind the hepatoduodenal ligament, and the Endoloop is ligated the distal end of the round ligament. (c) The Endoloop is pulled to the right upper abdomen through the abdominal wall and fixed by forceps. (d) The hepatic resection underwent under the good surgical view and appropriate tension between the hilar plate and resected liver.
{kind=link}
Discussion
According to the IWATE criteria, segments 7, 8, and 1 are considered the most challenging resection sites [1], and securing a good surgical field is challenging if the resection line is located in the para-caval portion of the caudate lobe. In 2006, Dulucq first reported two cases of laparoscopic isolated resection of hepatic S1 [2]. Since the late 2000s, laparoscopic liver resections of the caudate lobes have gradually increased, and their safety and feasibility have been reported in various analyses [3–6]. A recent study reported that laparoscopic caudate lobectomy resulted in a lower amount of intraoperative estimated blood loss, similar postoperative complications, a lower rate of respiratory infection, and shorter postoperative hospital stay than the open method [6].
However, securing the operative field for laparoscopic liver resection, in which the paracaval portion of the posterior aspect of the hepatoduodenal ligament is the hepatic resection line, remains a major problem. Recently, several techniques, pitfalls, and methods have been reported to overcome these difficulties [7–14]. Chai et al. reported that ‘arantius ligament suspension’ effectively compresses the lateral lobe, secures the operative field, and achieve good exposure of the left portal pedicle or left posterior surface for a left-sided approach [10]. Zheng et al. reported a laparoscopic left-sided approach combined with counterclockwise dissection for tumors located in the caudate lobe [13]. Huang et al. reported an in-depth summary of the tips and pitfalls of laparoscopic caudate lobe resection [14]. However, reports on laparoscopic caudate lobectomy and isolated caudate resection, which are anatomically difficult sites, and their tips and pitfalls remain insufficient.
Furthermore, ‘the hepatoduodenal ligament lifting technique’ improves the surgical field on the posterior aspect of the hepatoduodenal ligament and provides appropriate tension between the hepatic hilar plate and liver. Additionally, this technique is adaptable to left- and right-sided approaches, convenient, stable, easy to reposition, protective for the hepatoduodenal ligament, enables easy adjustment of subtle force, and does not require an assistant. Therefore, it is a useful technique for laparoscopic liver resection in which the resection line is a para-caval portion of caudate lobe.
Acknowledgements
We thank Editage (www.editage.jp) for the English language editing.
Conflicts of interest
None declared.
Funding
None declared.
Comments